Primary Care Society of Gastroenterology Covid-19 update 20th March 2020
On 17th March 2020 the BSG emailed its members with the following advice:
We are all aware that the Covid-19 situation is putting undue pressure on all parts of the healthcare system; we mustn’t forget that patients will still develop other illnesses, including cancer. Gastroenterology is an area of medicine where stress can exacerbate many symptoms and it may be easy to dismiss abdominal pains and diarrhoea as either indirect symptoms of Covid-19 or those of IBS. We need to retain our clinical acumen and listen for those warning bells that alert us to underling disease that need investigation: unintentional weight loss, nocturnal defaecation, bloody diarrhoea, weight loss or new onset of IBS-symptoms in women over 501. Examining patients for hepatomegaly, abdominal or rectal masses is going to be harder than usual, but we should still find safe ways to do this where it is clinically necessary.
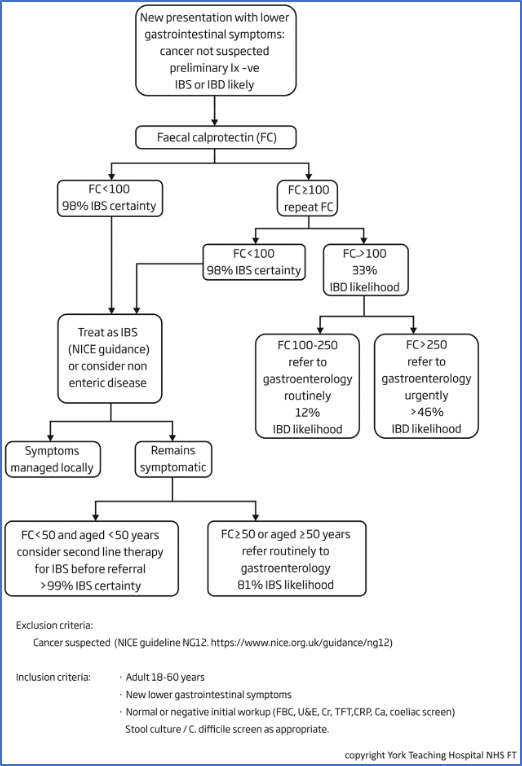
NICE DG11 (Figure 1)2 and the British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults3 (Figure 2) both have very similar guidance for the investigation of persistent (>4 weeks) lower abdominal symptoms in adults. In order to ensure that we are not overloading our secondary care colleagues we should follow these guidelines and avoid referring patients who do not need investigating. Those patients given a presumed diagnosis of IBS using these pathways and who have not responded to the therapies recommended in NICE CG614 may need referral, but the balance of risks to the patient of attending outpatients should be discussed and an appropriate balance struck.
Patients on immunosuppressive therapies may ask us for advice. The current UK Guidance on social distancing for everyone in the UK and protecting older people and vulnerable adults (updated 20th March 2020) states that those at risk, including those with “a weakened immune system as the result of conditions such as HIV and AIDS, or medicines such as steroid tablets or chemotherapy” should “significantly limit your face-to-face interaction with friends and family”. Further guidance is due out next week, but the guidance is not clear: which immunosuppressant medications or combinations of medications put one at greater risk, and what dose of corticosteroid causes significant immunosuppression? NICE CKS and the BNF state that a physiological dose is “about 7.5 mg of prednisolone or equivalent” therefore it would be pragmatic to take this daily dose as a cut-off. Crohn’s and Colitis UK5 are providing advice for patients, and the NHS guidance (released 19th March 2020) for rheumatology units can help us give general advice to patients on immunosuppressive therapies6, many of which will also apply to patients being treated for gastrointestinal conditions.
In essence, the risk of a flare of disease and the subsequent immunosuppression from this and the potential high doses of oral steroids needed to bring this under control would outweigh the risk from maintaining the vast majority of patients on their current medication regimes.
NHS England has promised more guidance next week, but I hope that this update has provided some reassurance that we can look after our patients with gastrointestinal problems in primary care.
Stay safe, maintain an appropriate social distance where possible, and keep washing your hands!
Kevin Barrett
Chair of the Primary Care Society of Gastroenterology
References
- https://www.nice.org.uk/Guidance/DG11
- https://www.nice.org.uk/guidance/ng12/chapter/1-Recommendations-organised-by-site-of-cancer#lower-gastrointestinal-tract-cancers
- Lamb CA, Kennedy NA, Raine T, et al British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adultsGut 2019;68:s1-s106.
- https://www.nice.org.uk/Guidance/CG61
- https://www.crohnsandcolitis.org.uk/news/coronavirus-covid-19-advice
- https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/clinical-guide-rheumatology-patients-v1-19-march-2020.pdf
Figure 1: NICE DG11 Faecal calprotectin diagnostic tests for inflammatory diseases of the bowel1
{kind=link}